

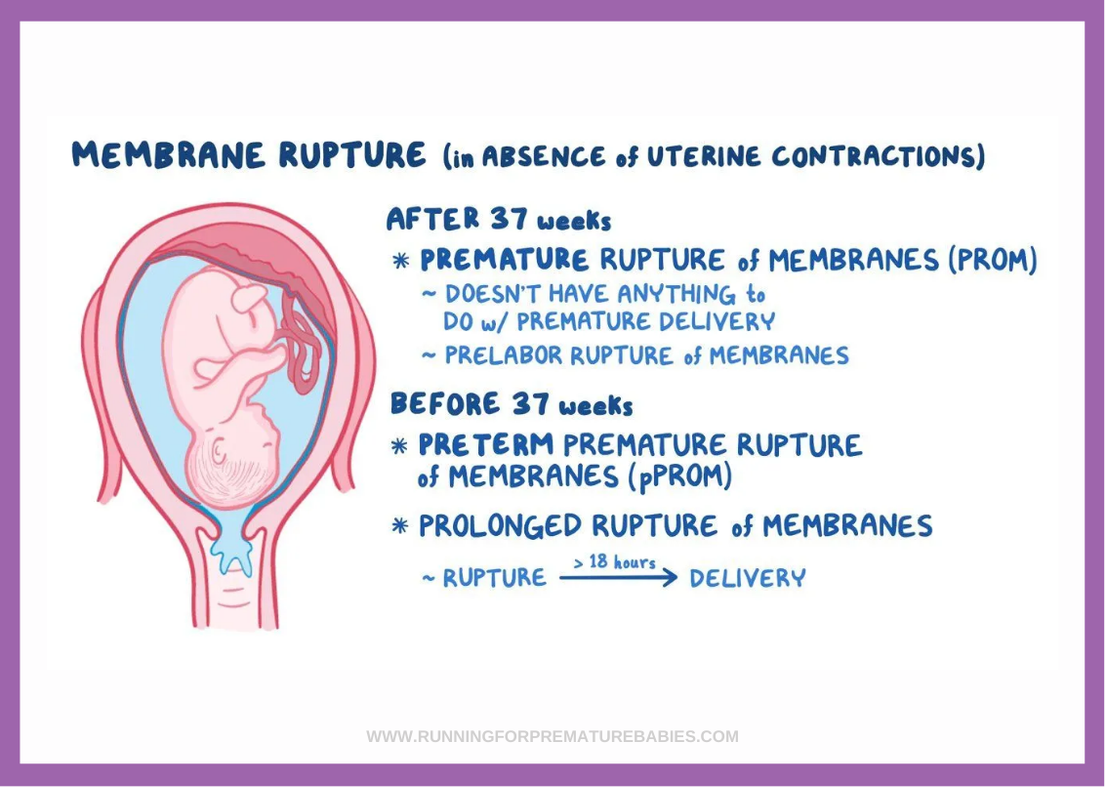
Preterm Prelabour Rupture of Membranes (PPROM)
A Quick Guide
If you experience PPROM symptoms during pregnancy such as fluid loss or pelvic pressure seek medical help immediately. Preterm prelabour rupture of membranes can pose risks for both mother and baby.
What is PPROM?
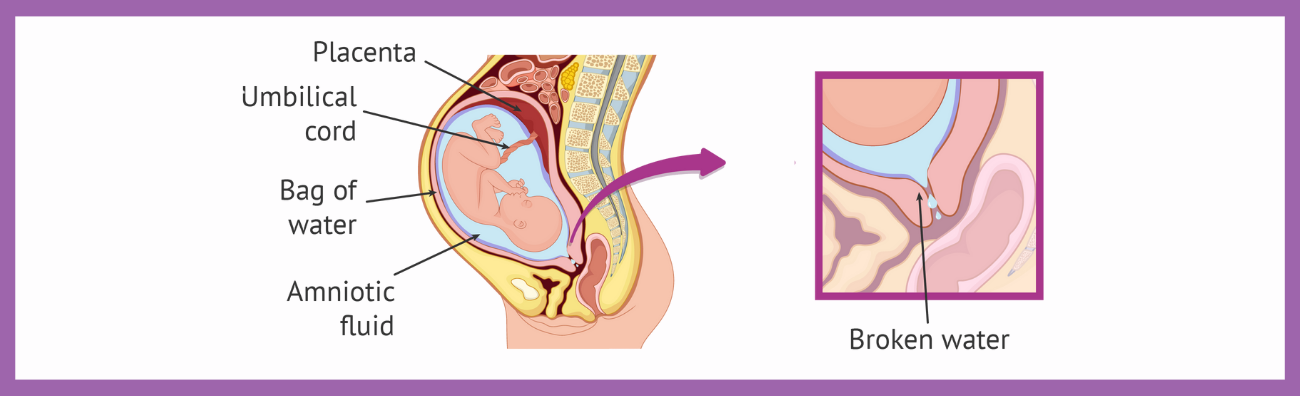
Preterm Prelabour Rupture of Membranes (PPROM) occurs when the amniotic sac around the baby ruptures before 37 weeks of pregnancy and before labour begins. It is a leading cause of preterm birth and is associated with maternal, foetal, and neonatal complications.
Does PPROM cause premature birth?
PPROM significantly increases the likelihood of premature birth, with clinical management focused on reducing complications and improving neonatal survival. Data from The Royal Hospital for Women NSW indicates PPROM complicates up to 3% of pregnancies and accounts for 30-40% of preterm births. More recent studies indicate 70-90% of women with PPROM go into labour within seven days, leading to preterm birth.
What causes PPROM?
PPROM is often caused by a combination of infection, inflammation, and structural factors that weaken the amniotic sac or membrane. In some cases, the exact cause is unclear, which is why it is important to be aware of the possibility.
- Infections – Bacterial infections in the uterus or lower genital tract can lead to membrane weakening.
- Inflammation – can contribute to premature rupture.
- Placental abruption or separation – Early separation of the placenta increases the risk of PPROM.
- Cervical insufficiency – A weakened or short cervix may fail to continue to support the pregnancy, leading to membrane rupture.
- Polyhydramnios (Excess amniotic fluid) – can puts pressure on the membranes.
- Multiple pregnancies – Twin or triplet pregnancies can increase strain on the uterus.
- Previous PPROM or preterm birth – A history of PPROM raises the likelihood of recurrence by around 20-30%. . While this is a high recurrence risk compared to the general population (where PPROM occurs in only 1–3% of pregnancies), most women with a history of PPROM will still deliver at term in their next pregnancy.
- Invasive procedures – Amniocentesis, chorionic villus sampling, or cervical cerclage can increase the risk of PPROM
- Smoking – Is linked to membrane weakening and early rupture. It nearly doubles the risk.
This information has been reviewed by Neonatologist, Dr John Smyth MBChB, FRACP FRCPCH.
Disclaimer: This information by Running for Premature Babies Foundation is educational and informative in nature and is not medical advice or a healthcare recommendation. For further information, please Contact Us.
See FAQs Below
Get Involved
Run with us
Donate
Join the Premmie Marathon Challenge

The vital role of research
Whilst relatively rare, research indicates placenta praevia cases are on the rise in correlation with increased caesareans. Charities such as Running For Premature Babies play a vital role in funding essential medical research, focused on pre- and post-natal care. Continued advancements in screening tools and ongoing research could significantly improve outcomes for mothers affected by placenta praevia, giving babies a better chance of survival.
At Running for Premature Babies, we are incredibly grateful for our dedicated community of fundraisers and volunteers. If you’d like to support research into preterm birth or complications like placenta praevia, including studies into the classification of placenta praevia, your donation can make a lasting impact. Help equip hospitals with essential NICU resources by donating here.
FAQs
How common is PPROM in Australia?
PPROM is responsible for 30-40% of preterm births in Australia and occurs in approximately 2-4% of singleton pregnancies and 7-20% of twin pregnancies.
What happens if PPROM happens before 24 weeks?
What are the survival rates of babies born after PPROM?
PPROM Survival rates vary depending on gestational age at rupture and medical intervention.
22-23 weeks: Neonatal mortality remains high, with up to 60% of babies not surviving.
24-28 weeks: Survival rates increase significantly with each week , with up to 70% of babies surviving at 24 weeks gestation and 70-80% at 25 weeks if they are born in a specialised centre. Survival at 26-28 weeks gestation is 80-90+%.
28-33 weeks: Survival rates increase significantly, with most babies surviving.
Ref:
Min et al. Risk of recurrent preterm premature rupture of membrane in subsequent pregnancy: a systematic review and meta-analysis. J Maternal-Fetal & Neonatal Medicine 2026
What Neonatal care is needed for PPROM babies?
In Australia, neonatal care for babies born after PPROM focuses on infection prevention/antibiotic therapy, respiratory support, and feeding/developmental care. Hospitals follow structured PPROM guidelines to reduce complications and support long-term outcomes.
References
A?ao?lu, R.T., Öztürk, Ö., Ulusoy, C.O. et al. Perinatal outcomes and predictors of neonatal mortality in preterm premature rupture of membranes: a tertiary centre experience. BMC Pregnancy Childbirth 25, 585 (2025). Retrieved 29th May 2025 https://doi.org/10.1186/s12884-025-07688-9
The Royal Hospital for Women, Local Operating Procedure (2016) Retrieved 29th May 2025 https://www.seslhd.health.nsw.gov.au/sites/default/files/documents/pprom2016.pdf
NSW Government Management of Threatened Preterm Labour (2022) Retrieved May 29th 2025 https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/GL2022_006.pdf
Safer Care Victoria. (n.d.). Preterm pre-labour rupture of membranes. Retrieved 29th May from https://www.safercare.vic.gov.au/best-practice-improvement/clinical guidance/maternity/preterm-pre-labour-rupture-of-membranes
Laura Goodfellow, Angharad Care, Ciara Curran, Devender Roberts, Mark A Turner, Marian Knight, Alfirevic Zarko - Preterm prelabour rupture of membranes before 23 weeks’ gestation: prospective observational study: BMJ Medicine 2024;3:e000729. Retrieved 29th May https://bmjmedicine.bmj.com/content/3/1/e000729

